術前
 多分、歯頸部の充填物が脱離して、虫歯にもなってます。
多分、歯頸部の充填物が脱離して、虫歯にもなってます。
術中

(以下、すべてマイクロスコープを使用しています。)虫歯の部分を除去し、レジン充填を行う準備を行なっています。

まずは、黒の糸をいれて更に、その上から白い糸を入れてます。これは詰め物が、段差なく移行的にするための前処置です。
 レジン充填を行いました。(色が黄色いのはフィルターをかけてます。)その後、糸を取り除きます。
レジン充填を行いました。(色が黄色いのはフィルターをかけてます。)その後、糸を取り除きます。
術後
 綺麗にできたと思います。大切なことは、色が合っていることもですが、段差も見られないことが大切です、
綺麗にできたと思います。大切なことは、色が合っていることもですが、段差も見られないことが大切です、

広島県福山市の歯科医院

多分、歯頸部の充填物が脱離して、虫歯にもなってます。
(以下、すべてマイクロスコープを使用しています。)虫歯の部分を除去し、レジン充填を行う準備を行なっています。
まずは、黒の糸をいれて更に、その上から白い糸を入れてます。これは詰め物が、段差なく移行的にするための前処置です。
レジン充填を行いました。(色が黄色いのはフィルターをかけてます。)その後、糸を取り除きます。
綺麗にできたと思います。大切なことは、色が合っていることもですが、段差も見られないことが大切です、

まあ、このテクニックはお口の中のフッ素濃度を長く保つことがミソなのでしょうか?
実践するとわかりますが、歯磨き粉の量が多いわりにすすぎの水の量はすくなく、市販の歯磨き粉で行うと余りにさわやかで、、、、就寝前に行うと寝れないかも?
ということでより実践的に Check-Up gel(ライオン)をお勧めします。
よく読むとイエテボリテクニックとよく似ていると思います。狙いは一緒でしょう。これだと特に子供の場合、味もきつくなくすすんでブラッシングができるようになると思いますし、フッ素濃度もきちんとそれように考えられているのでお勧めです。
レントゲンの被爆について
”シーベルト”という単位を最近よく聞くようになりました。
レントゲンを撮影する場合、X線を当てて撮影します。このとき、人体は放射線にさらされます。これを”放射線被爆”といいます。大量の放射線被爆は人体に有害です。ただどの程度の被爆にさらされるかが問題でその尺度として”シーベルト”という単位が用いられます。
一般に、100mSvが健康被害が出始める被爆量なので歯科用レントゲンでの被爆はほぼ問題ないとおもわれます。さらに、鉛入りのエプロンで防御もしますので実質の被爆量はさらに減ります。
|
実効線量 (mSv)
|
内訳
|
|
0.1 – 0.3
|
1回の胸部X線撮影。
|
|
0.2
|
東京とニューヨーク間を航空機で1往復 (高度での宇宙線増加)。
|
|
1.0
|
一般公衆が1年間にさらされてよい人工放射線の限度
放射線業務につく人 が妊娠を知ったときから出産までにさらされてよい放射線の限度
|
|
6.9
|
CT検査1回での被爆量
|
|
10
|
日本国原子力安全委員会の指針での一般人の「屋内退避」
ブラジル・ガラパリで1年間に自然環境から1人が受ける自然放射線。 |
|
0.01 – 0.04
|
パノラマX線(大きな口腔内全体を撮影)撮影での被爆量
|
|
0.001 – 0.004
|
デジタルパノラマX線(大きな口腔内全体を撮影)撮影での被爆量
|
|
0.01 – 0.03
|
デンタルレントゲン(数歯単位の小さな)の撮影
|
|
0.001 – 0.003
|
デジタルデンタルレントゲン(数歯単位の小さな)の撮影
|


 ”隠し文字”って知ってました?いままで知らなかったというか、日本のお札の印刷技術はすごい!!1000円の桜のなかに”ニ”、”ホ”、”ン”の文字が見えます。黄色丸の中に”ホ”の字が見えます。
”隠し文字”って知ってました?いままで知らなかったというか、日本のお札の印刷技術はすごい!!1000円の桜のなかに”ニ”、”ホ”、”ン”の文字が見えます。黄色丸の中に”ホ”の字が見えます。
マイクロスコープでははっきり見えますが、裸眼では歳のせいか無理でした、、皆さんも見てみてください。(他にも隠し文字はあります。)

 典型的な反対咬合です。この症例では、年齢を考慮して”シールド”の使用をお勧めしました。(2012.7.18)
典型的な反対咬合です。この症例では、年齢を考慮して”シールド”の使用をお勧めしました。(2012.7.18)
 まだ4か月程度ですが、かなり改善されてきたと思います。永久歯の生えてくる前に改善すれば、上顎骨の成長を妨げなくなりますし、また顔貌もしっかりしてきます。(2012.10.23)
まだ4か月程度ですが、かなり改善されてきたと思います。永久歯の生えてくる前に改善すれば、上顎骨の成長を妨げなくなりますし、また顔貌もしっかりしてきます。(2012.10.23)

ひさびさに来院されました。(2013.8.16)途中来院が途絶えて、久々の経過観察なのですが、立派に直りました。経過観察が途絶えたこともあり、やや使い過ぎなきもしますが、まあいいのではないでしょうか。あとは、永久歯になってもこの状態が保てるか慎重に経過をみなければなりません。

 マイクロスコープを使うと、はっきりとものが観察できます。真ん中のピンク色に見えるものが、ガッターパーチャーと呼ばれる根充材です。面白いことに、この症例では、一般的な歯と頬舌側が反対でしたが、マイクロスコープを使用しての根管治療でしたので、自信をもって処置が行えました。
マイクロスコープを使うと、はっきりとものが観察できます。真ん中のピンク色に見えるものが、ガッターパーチャーと呼ばれる根充材です。面白いことに、この症例では、一般的な歯と頬舌側が反対でしたが、マイクロスコープを使用しての根管治療でしたので、自信をもって処置が行えました。
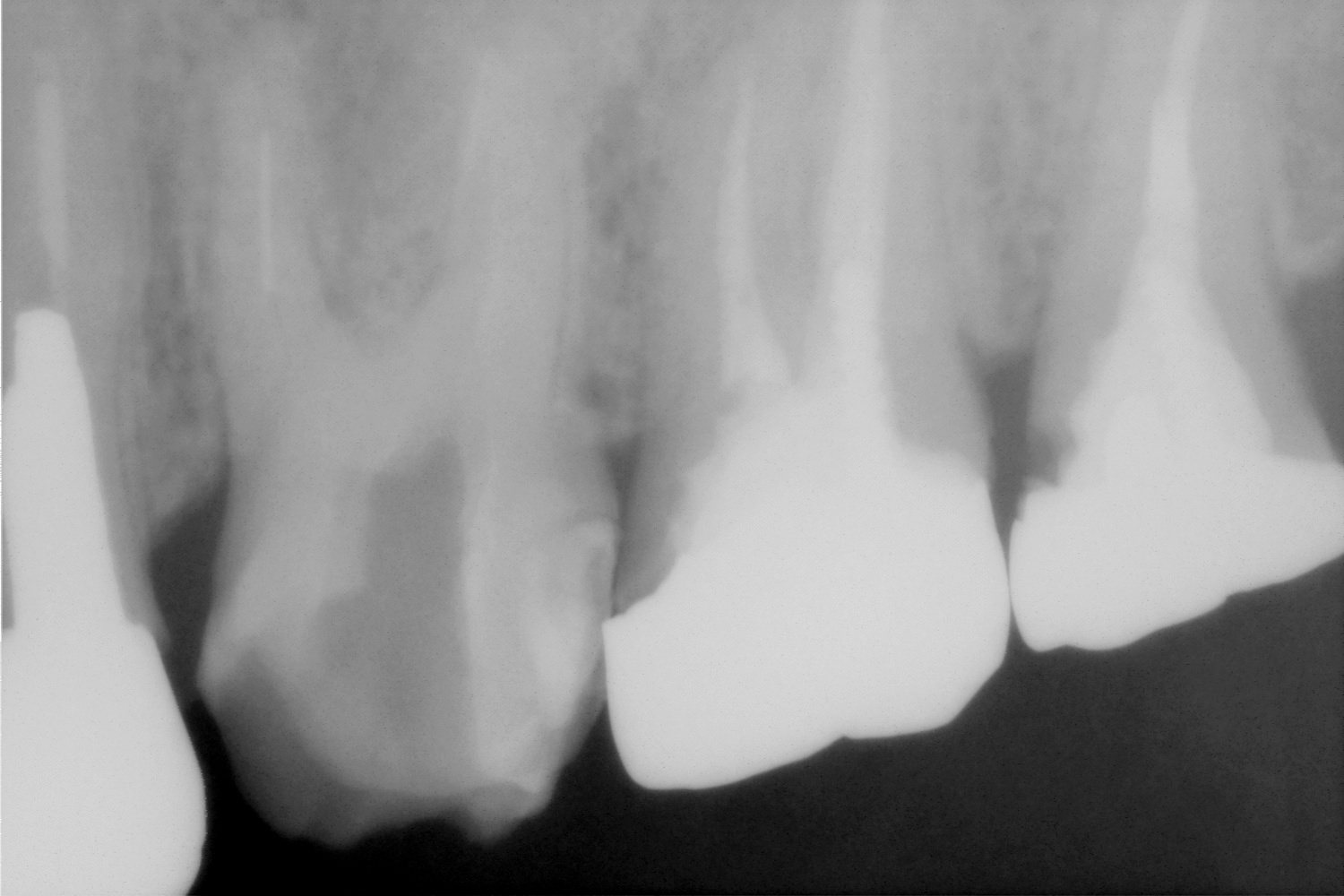
 左上の6番近心頬側根に何かあります。そこそこ、深く細いのですが、なんとか、除去し、治療を続けました。この根管は腫れやと痛みの原因になっていたので、除去できなければ、抜歯もしくは抜根等の外科処置もしくは抜歯が必要でした。
左上の6番近心頬側根に何かあります。そこそこ、深く細いのですが、なんとか、除去し、治療を続けました。この根管は腫れやと痛みの原因になっていたので、除去できなければ、抜歯もしくは抜根等の外科処置もしくは抜歯が必要でした。
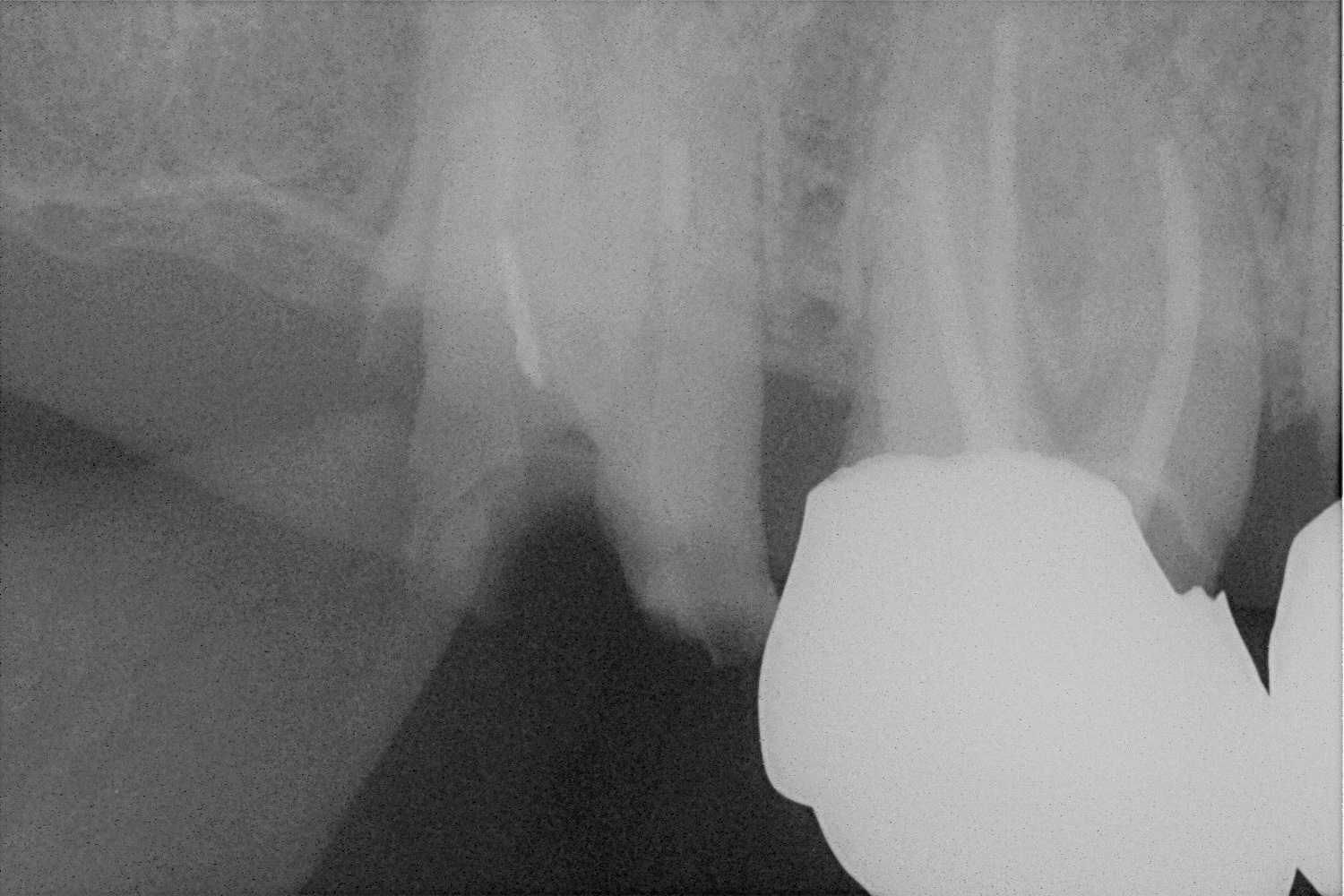
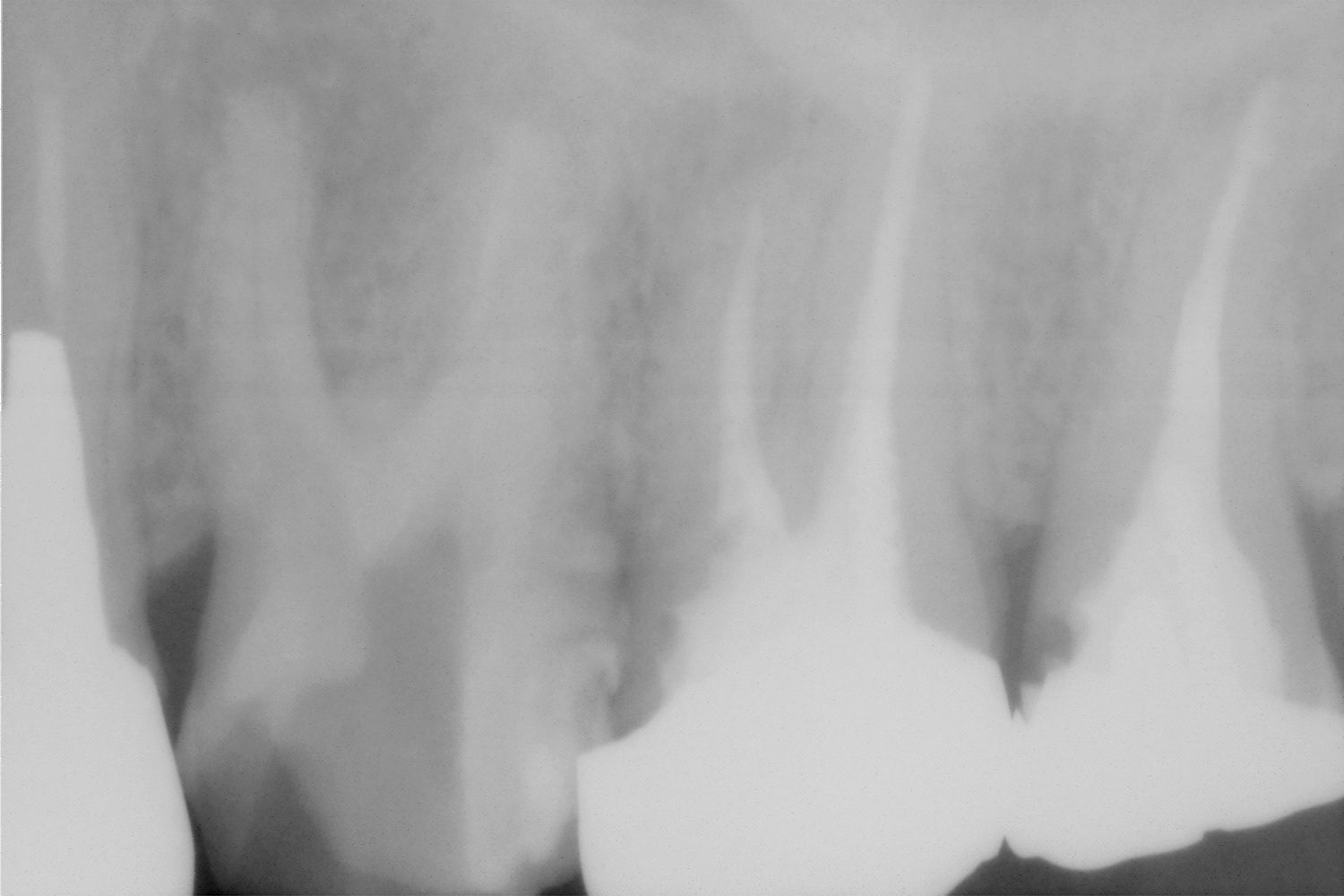 無事に除去できました。レントゲンからわかるように、無駄な拡大もおこなっていないと思います。
無事に除去できました。レントゲンからわかるように、無駄な拡大もおこなっていないと思います。



マイクロスコープを使用して除去しました。
これは、そこそこ深いところにありましたが、マイクロスコープにて除去できました。
 根っこの中に、なにかギザギザなものが見えますが、、裸眼の治療ではちょっと除去不可能です。
根っこの中に、なにかギザギザなものが見えますが、、裸眼の治療ではちょっと除去不可能です。
マイクロスコープを使用して除去しました。
なにやら、見えますが、これで安心して治療が続けられますね。

Allan S. Deutsch, D.M.D.
Quick Factoid: Endo vs. Implants
January – March 2009How will general dentists doing root canals react? It is reported that
someare bypassing endo altogether and going straight to single-tooth implants. The indications,treatment planning, and considerations are varied; what is your reaction? You can reach me at:adeutsch@edsdental.com.
Comparison of Success of Implants Versus Endodontically Treated Teeth
J. P. Hannahan and P. D. Eleazer
Implants versus root canal therapy is a current controversy in dentistry. The purpose of this investigation was to compare the success of each treatment, with minimal subjective grading. Outcome was determined by clinical chart notes and radiographs. Failure was defined as removal of the implant or tooth. Uncertain findings for implants were defined as mobility class I or greater, radiographic signs of bone loss, or an additional surgical procedure. Mobility, periapical index score of 3 or greater, or the need for apical surgery was classified as uncertain for endodontically treated teeth. Success was recorded if the implant or tooth was in place and functional. Implants were placed by periodontists in a group practice, whereas the endodontic treatments were performed by endodontists in group practice. Charts of 129 implants meeting inclusion criteria showed follow-up of an average of 36 months (range, 15-57 months), with a success rate of 98.4%. One hundred forty-three endodontically treated teeth were followed for an average of 22 months (range, 18-59 months), with a success rate of 99.3%. No statistically significant differences were found (P = .56). When uncertain findings were added to the failures, implant success dropped to 87.6%, and endodontic success declined to 90.2%. This difference was not statistically significant (P = .61). We found that 12.4% of implants required interventions, whereas 1.3% of endodontically treated teeth required interventions, which was statistically significant (P = .0003). The success of implant and endodontically treated teeth was essentially identical, but implants required more postoperative treatments to maintain them.
A topic that seems to be coming up more and more is “endodontics versus implants, when to do which?” More and articles are being written on the success of endo versus implants.
The article below was published in the November 2008 issue of the Journal of Endodontics.
まあ、簡単に読むとインプラントも根管治療も成功率は変わらないけどインプラントはプロフェショナルなお手入れをしっかりねという内容だと思います。なら、治せるなら根管治療したほうが、いいんじゃない?と思いますがいかがでしょう。